
Published on July 13, 2026
Diseases affecting egg quality: a technical review
Egg quality is a key parameter of commercial layer performance, influencing profitability, animal welfare, and food safety. Many infectious agents disrupt the physiology of the reproductive tract or the bird’s overall health, resulting in eggshell defects, internal egg abnormalities, and significant production declines.
Egg formation is a delicate and complex process that spans approximately 24 hours. It begins with the release of the follicle (ovulation) which will be captured by the infundibulum, followed by the secretion of albumen in the magnum: this process takes about 3 to 4 hours. The egg then progresses to the isthmus, where shell membranes are formed in about 1 hour. Next, the egg enters the uterus (shell gland), where hydration of the albumen, calcification, pigmentation, and cuticle deposition occur. Finally, the fully formed egg is released through the vagina, and finally the cloaca (oviposition).
Because this process involves multiple tissues and hormonal pathways, any systemic infection or localized damage to the reproductive tract can lead to diminished egg quality. Genetics, nutrition, management and environmental conditions also have major impacts on egg quality, but this article reviews only the most relevant infectious diseases affecting egg quality in laying hens. Understanding the pathophysiological mechanisms of these diseases is fundamental to improving prevention strategies, optimizing vaccination programs, and ensuring consistent production performance.
Infectious Bronchitis (IB)
Infectious Bronchitis, caused by a Gammacoronavirus with high mutation and recombination potential, is one of the most important viral threats to egg quality. The virus shows strong affinity not only for the respiratory tract but also for the kidneys, digestive tissues, and, critically, the reproductive system. Its ability to rapidly generate variant strains complicates both diagnosis and vaccination.
Transmission occurs primarily through aerosols and contaminated droplets, enabling extremely rapid spread among birds. Contaminated drinking water and feed are additional routes, and manure transport from infected farms has been reported to disseminate the virus between flocks.
Respiratory symptoms are the most recognizable, including coughing, sneezing, nasal discharge, and dyspnoea. However, in laying hens the most economically damaging effect is the disruption of egg production. Laying hens may experience a sharp decline in lay, which can persist for six to eight weeks before returning to pre‑infection levels. The severity of this impact is strongly influenced by co-infections with pathogens such as Mycoplasma gallisepticum, Mycoplasma synoviae, E. coli, Avibacterium paragallinarum, or low‑pathogenic avian influenza strains.
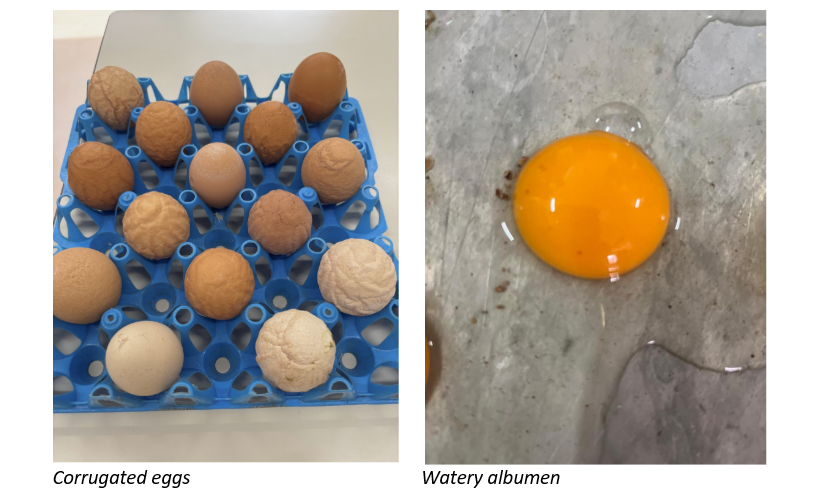
IBV-induced oviduct damage directly compromises shell formation and albumen quality. Affected eggs are frequently misshapen, rough, thin‑shelled, wrinkled and pale (in brown egg layers). Many eggs have watery albumen or exhibit internal defects such as blood or meat spots. A characteristic abnormality, associated with IBV, is the production of corrugated eggs. These arise when the process known as “plumping”,in which water is transferred to the albumen in the uterus to help shape the egg, is not properly finished.
Infection of young birds during rearing can permanently damage the oviduct. When these flocks reach sexual maturity, they may appear physiologically ready to lay (combs, wattles, opening of pelvic bones…), but egg production remains low. This condition is known as “False layer syndrome”. At post-mortem examination the oviduct is typically enlarged and filled with fluid.
Diagnosis of IB requires laboratory confirmation. ELISA tests are useful for detecting flock exposure but lack strain specificity; paired sampling is essential for assessing recent infection. HI tests provide serotype‑specific information, while RT‑PCR remains the most accurate tool for identifying circulating variants.
Control relies on strict biosecurity and well-designed and executed vaccination programs. Live attenuated vaccines induce rapid mucosal immunity and offer partial cross‑protection, while inactivated vaccines generate strong systemic antibody responses but little mucosal defense. Effective programs should combine both types and select the most prevalent virus types in the region, which can be challenging given the continual emergence of variants.
Newcastle Disease (ND)
Newcastle Disease, caused by Avian Paramyxovirus type 1, remains one of the most feared avian diseases due to its severe clinical manifestations and potential for substantial egg production losses. The disease has become enzootic in many parts of the world and has a significant impact on the poultry industry. The virus is classified in several pathotypes ranging from lentogenic strains causing mild enteric or respiratory infection to the highly virulent velogenic strains that cause high mortality.
Transmission occurs through direct contact with feces or respiratory secretions, or indirectly via contaminated equipment, litter, water or people. Although the virus can be inactivated by common disinfectants, it can persist for weeks in organic material. Vertical transmission is generally not viable because infected embryos die in the shell, but contaminated eggs can serve as sources of infection for newly hatched chicks.
Clinical signs depend on the pathotype, the immune status of the flock, and bird-age. Respiratory distress is common, including eye swelling, gasping, coughing, and rales. Neurotropic strains produce tremors, paralysis, and the classic twisted neck posture. Greenish diarrhea is frequently observed. In laying hen flocks, egg production usually drops, and eggs produced may be thin‑shelled, rough, pale, or irregularly shaped (e.g. mango shaped).
Lesions also vary with the strain and pathotype: tracheitis, pneumonia, and aerosacculitis frequently accompany respiratory disease, while virulent strains cause extensive hemorrhaging in organs such as the intestines, cecal tonsils, proventriculus-gizzard junction, and ovaries.
Because lesions are not pathognomonic, laboratory testing is essential for confirmation. Virus isolation and RT‑PCR are widely used, and serology, particularly HI testing, helps evaluate flock immunity and vaccination response.
Control depends on stringent biosecurity and vaccination. Live lentogenic vaccines are applied broadly to establish baseline protection, and inactivated vaccines are used to boost immunity and provide longer-term coverage. Recombinant HVT‑based vaccines can be administered at hatch but require additional live vaccination in high-challenge areas. Importantly, vaccination reduces clinical signs and mortality but does not fully prevent infection or viral shedding, underscoring the importance of strict biosecurity.

Egg Drop Syndrome (EDS)
Egg Drop Syndrome is caused by Duck Adenovirus 1, a member of the Atadenovirus group. Although the natural hosts for the virus are ducks and geese, it can infect chickens and cause significant reproductive dysfunction, particularly in brown egg layers, which tend to show more severe symptoms than white egg layers.
Transmission occurs through both vertical and horizontal routes. Breeder flocks infected with EDSV may transmit the virus to their progeny, leading to latent infections that remain unnoticed until the onset of lay. At this stage, the virus becomes activated, resulting in shedding and rapid spread through the flock. Horizontal transmission often occurs through contaminated eggs, egg trays, crates, or shared transport equipment. Massive viral replication takes place in the pouch shell gland region, directly affecting the bird’s ability to form normal shells.
EDS affected birds usually appear healthy, but eggs produced are pale, thin‑shelled, soft‑shelled, or shell‑less. Production may drop by 10 % to 40 %, but this loss is mainly because many malformed eggs are eaten by the hens, broken in the litter or lost on manure belts or in manure pits.
Diagnosis is based on clinical pattern recognition (sudden drop in lay with shell-less eggs in apparently healthy hens) and confirmed by laboratory tests such as ELISA, HI, and PCR. Effective control depends heavily on biosecurity and the avoidance of contaminated egg-handling equipment. Inactivated vaccines administered late in rearing are routinely used in breeders to prevent vertical transmission and are also applied in commercial layers to prevent clinical signs of disease, although they may not fully prevent viral shedding.

Avian Metapneumovirus (aMPV/SHS/TRT)
Infection with Avian Metapneumovirus in laying hens primarily manifests as a respiratory disease accompanied by reproductive disorders. There are several subtypes of the virus which replicate mainly in the epithelial cells of the upper respiratory tract, where it damages cilia and reduces mucociliary clearance, which increases susceptibility to secondary infections.
Transmission occurs through direct contact and aerosol exposure. Although the virus can be isolated from the reproductive tract, there is no evidence of vertical transmission.
The severity of clinical disease is influenced by environmental factors such as ventilation quality, and by the presence of secondary pathogens including Mycoplasma spp. and E. coli. Respiratory symptoms range from nasal discharge and watery eyes to sneezing and swelling of the infraorbital sinuses. However, in some flock respiratory signs are minimal, and the main observation is a sudden drop in egg production accompanied by egg quality defects. Brown egg layers tend to be more susceptible than white egg layers, particularly during the physiologically demanding period around peak of lay.
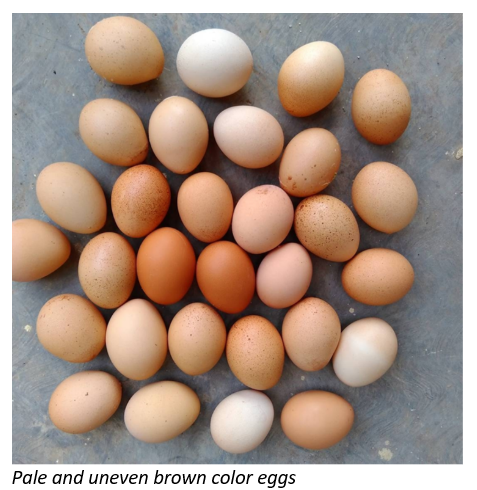
Egg quality defects typically include pale eggs, uneven shell coloration, and fragile shells. Misshapen eggs are less common than in IBV or NDV infections. Diagnosis employs ELISA testing, although limited cross‑reactivity between subtypes may difficult interpretation unless homologous antigens are used. RT‑PCR offers greater precision.
Control requires a combination of strict biosecurity, proper management of predisposing factors like ventilation, and vaccination. Live vaccines provide local immunity, while inactivated vaccines help extend protection through the laying period. Importantly, cell-mediated immunity appears to be more relevant for protection than antibody titers, meaning serological monitoring must be interpreted cautiously. Antibiotics can assist in controlling secondary bacterial infections but have no effect on the virus itself.
Mycoplasma synoviae: Egg Apex Abnormalities (EAA)
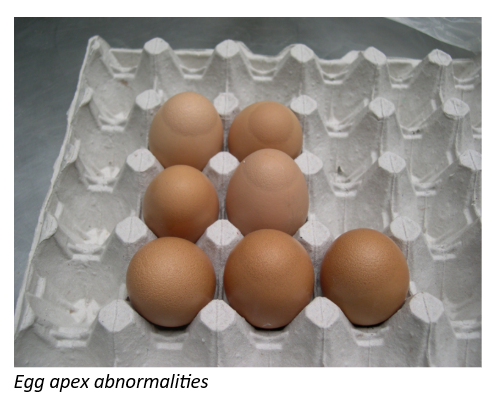
Mycoplasma synoviae is a small, rudimentary wall‑less bacterium with different strains of variable virulence having tropism for joints, the respiratory tract, and the reproductive system. This pathogen is known for producing a condition named Egg Apex Abnormality (EAA) or glassy pointed eggs, in which the apex of the egg becomes thin, translucent and structurally weak. These abnormalities can lead to significant egg rejection rates, sometimes reaching up to 20 % percent, and become particularly severe when MS infection occurs concurrently with Infectious Bronchitis virus (IBV).
Mycoplasma synovia is vertically transmitted. Horizontal transmission between farms is strongly linked to human activity via fomites (shoes, equipment…) or movement of infected carrier birds. The organism survives for only short periods in the environment, but up to 3 days and beyond on feathers.
Clinical signs may be mild, though respiratory signs or synovitis can occur depending on the strain’s virulence. Strains targeting the oviduct interfere with shell formation producing reduced eggshell quality specifically at the pointed end of the egg. Diagnosis relies on screening tests such as RPA or ELISA, with HI tests used to confirm suspicious results. PCR provides rapid, sensitive, and specific detection.
Control strategies include strict biosecurity protocols, the avoidance of multi-age systems, and targeted treatment using approved anti-mycoplasmal drugs (tetracyclines, macrolides…). However, antibiotics generally suppress clinical signs and reduce shedding rather than eliminating infection. Vaccination is available: the live temperature‑sensitive MS‑H vaccine is widely used administered via eye drop. Flocks must be free of the pathogen before vaccination, and the vaccine strain can be differentiated from field strains by PCR.
Other diseases impacting egg quality
Low-pathogenic avian influenza H9N2 can cause oviduct lesions that result in thin-shelled eggs. Other respiratory infections such as Infectious Laryngotracheitis or Coryza may reduce overall hen health and thereby compromise egg formation. Intestinal diseases including necrotic enteritis or Brachyspira infections impair nutrient absorption, leading to pale eggs or altered yolk discoloration. Heavy worm infestations have been reported to cause reduction in eggshell color, and, in rare cases, worms may even be found inside the egg.
Conclusion
Egg quality is highly vulnerable to a wide range of infectious agents, many of which affect not only the reproductive tract but also the respiratory, digestive, and metabolic systems of laying hens. Ensuring optimal egg production requires a multifaceted approach that integrates strict biosecurity, well-designed vaccination programs, careful monitoring of environmental and management factors, and timely diagnosis when abnormalities appear. Because egg formation depends on the hen’s overall physiological balance, any disruption (infectious or otherwise) especially when daily feed intake is affected, can negatively impact egg quality and production outcomes. When effective prevention, sound day-to-day management in rearing and production, and flock health align, a laying hen can fully express her genetic potential, turning egg quality from a point of vulnerability into a consistent and reliable strength throughout her productive lifetime.


